

Introduction:
Relapsed/refractory AML and MDS present a clinical challenge. Despite FDA approval of multiple new targeted agents, many patients lack actionable mutations and have exhausted conventional chemotherapeutic options. We have shown that NK cell infusions after lymphodepleting chemotherapy can induce remissions in relapsed/refractory AML. However, this cell-based therapy lacks antigen specificity. To address this, we developed GTB-3550 TriKE, a novel CD16/IL-15/CD33 Tri-Specific Killer Engager (TriKE). GTB-3550 TriKE is comprised of two single chain variable fragments (scFvs); one that binds CD16 on NK cells and one that binds CD33 on myeloid malignancies, plus an IL-15 linker bridging the CD16 and CD33 scFvs for sustained cell activation. Pre-clinical data shows specific NK cell activation and targeted cytolytic activity in xenogeneic AML mouse models.
Methods:
Patients with CD33+ malignancies (primary induction failure or relapsed AML with failure of one reinduction attempt or high risk MDS progressed on two lines of therapy) age 18 and older were eligible (NCT03214666) if they had adequate renal, hepatic, cardiac and lung function and absolute lymphocyte count (ALC) ≥ 200 cells/µL or absolute circulating CD56+/CD3- NK cell count >25 cells/µL within the 14 days prior to start of therapy. The primary endpoint is to identify the maximum tolerated dose (MTD) of GTB-3550 TriKE. Correlative objectives include the number, phenotype, activation status and function of NK cells and T cells.
During phase 1, each patient received the GTB-3550 TriKE at 5-200 mcg/kg/day (in 6 cohorts) for 3 weeks (infusion block #1, #2, and #3) of 96 hours continuous infusion separated by a 72-hour rest. Two patients enrolled per dose cohort. Disease response assessed by bone marrow biopsy between Days 21-42.
Results:
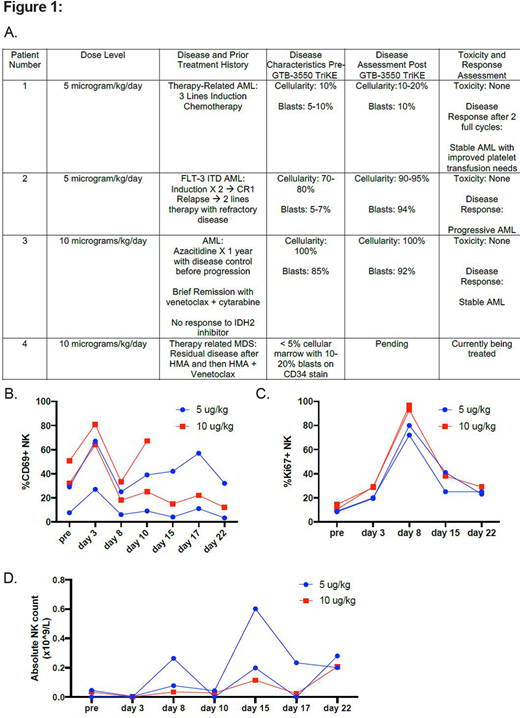
Four patients have enrolled, two at 5 mcg/kg/day and two at 10 mcg/kg/day, and three have completed therapy. Two patients with stable disease and one had substantial disease progression in the setting of a FLT-3 ITD mutation (Figure 1A). The first patient at 5 mcg/kg/day had stable disease after course 1 and qualified for retreatment with a second course of 3 weeks of GTB-3550 TriKE due to improved platelet transfusion requirements. Of the four complete courses of treatment delivered, all were delivered on schedule without treatment interruptions. The previous MTD of continuous infusion rhIL-15 was 2 mcg/kg/day (Conlon et al, Clin. Ca Res.) with associated fevers, tachycardia and constitutional symptoms. Validating our pre-clinical data showing decreased IL-15 potency when sandwiched between the CD16 and CD33 scFvs, patients treated with GTB-3550 TriKE treatment displayed no signs of clinical immune activation or SAE's in the 5 and 10 mcg/kg/day cohorts.
Correlative studies have shown reproducible NK cell activity in all patients. NK cell activation (CD69+) increases early during treatment (Figure 1B). The greatest NK cell proliferation (Ki-67+) starts at day 3, is maximal at Day 8, and maintained above baseline at Day 15 and Day 22 (Figure 1C). This correlated with an increase proportion and absolute number of NK cells during treatment (Figure 1D). Targeted delivery of IL-15 to NK cells through the anti-CD16 engager showed preferential proliferation of NK cells and significantly less effect on CD8+ T cells. Additionally, the frequency of NK cells and absolute lymphocyte count decreased early during the continuous infusion of the GTB-3550 TriKE, which rebounded after the 72-hour rest period to higher levels than the pre-treatment baseline.
Conclusion: This novel GTB-3550 TriKE administered by continuous infusion led to NK cell proliferation in all patients at initial dose levels and no clinically significant targeted toxicity. Though no objective responses were seen at the initially low dose cohorts tested, these early data suggest proof of principle that the drug has immune activity in humans. Subsequent patients given higher dose levels will determine if NK cell proliferation translates into clinical efficacy.
Weisdorf:Incyte: Research Funding; FATE Therapeutics: Consultancy. Vallera:GT Biopharma: Consultancy, Patents & Royalties, Research Funding. Schroeder:GT Biopharma: Consultancy, Current equity holder in publicly-traded company. Felices:GT Biopharma: Consultancy. Miller:Fate Therapeutics, Inc: Consultancy, Patents & Royalties, Research Funding; GT Biopharma: Consultancy, Patents & Royalties, Research Funding; Vycellix: Consultancy; Onkimmune: Honoraria, Membership on an entity's Board of Directors or advisory committees; Nektar: Honoraria, Membership on an entity's Board of Directors or advisory committees.
GTB-3550 TriKE is a cytokine immune engager binding to CD16 on NK cells, CD33 on myeloid blasts and IL-15 between the two engager components.

